I spend a lot of time talking to migraine and fibromyalgia sufferers from all over the world, talking to them via email or Facebook or blog–some even phone. I consistently find–particularly in the Unites States–that anxiety related conditions are treated with antidepressants. This was very clear to me when I was a migraine sufferer and my migraine specialist wanted to place me on a serotonin preventive as she explained it is for depression but seems to work for many people with migraines.
This sent me to research the subject and of course it ended up in a book with a solution for migraine, finding the cause–which by the way shows that migraines have nothing to do with depression. I am very happy that I turned away from the serotonin preventive and in fact turned away from all migraine medications since they were all some form of triptans, which are serotonin.
As now my book on migraine is quite successful and many people are cured completely without any medications, I can stop and look why exactly are triptans offered for migraine when originally they are antidepressants. Is there a logical connection anywhere that I missed when I attended my doctoral classes on the brain? Have I missed the brain anatomy to such large degree that I cannot tell regions of anxiety and regions of depression apart? What exactly does the research community have available to make the statement that antidepressants will work on anxiety? And on those occasions when they actually do work–as sometimes they do–why do they work? And why don’t they work other times?
In this article I compare brain anatomy by pictures available on the Internet–I will be citing all publications and provide links so you can follow and read. Let me start by a couple of pictures of depression so you can see where in the brain the light areas are, which represent areas that were affected by depression when they did not light up.
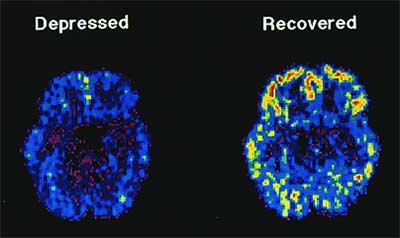
PET scan depression
This picture was taken from the website linked above. Here you can see on the PET-scan that the areas affected by depression are on the outskirts of the brain, following the serotonin pathways.
serotonin pathways
The above picture was taken from the link marked under “serotonin pathways” above. Dopamine is also included on this particular picture. The picture is excellent because it explains what functions dopamine and serotonin have and what they are responsible for. Note that neither indicates any connection to anxiety. In fact, in terms of anatomy, the areas responsible for anxiety are not even highlighted on any of these two pictures!
The questions necessarily arise: where are the anxiety sensitivity regions on the map? And if they are not connected to the depression part of the brain, why are anti-depression medications prescribed for anxiety?
The areas of the brain in anxiety disorder are well discussed in this article and the picture below shows a good description of the anatomy and the flow direction of anxiety response, part of the same article, here I post separately in case you don’t want to read the above article linked to:
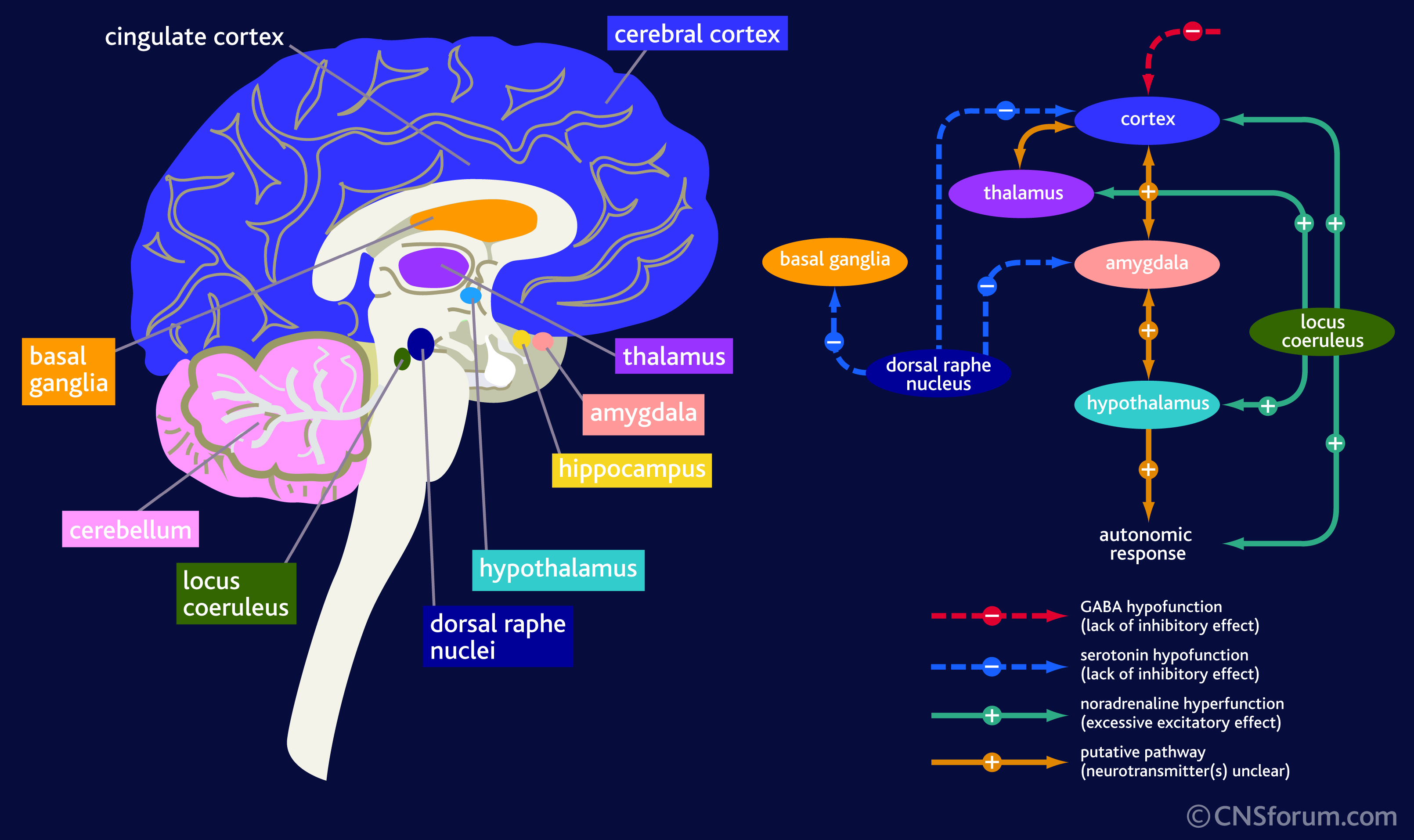
anxiety disorder picture
The picture above has 2 parts. On the left it shows of the many colors of various brain parts. One tiny green dot called the Locus Coeruleus is responsible for anxiety, which is an extension of the limbic system of the brain (often referred to incorrectly as the reptilian brain). Note that this particular part of the brain is separate from those that are affected by depression.
On the right there is an important table. It shows the path that anxiety takes as it manifests itself. It starts in the Locus Coeruleus and then heads into the cortex (blue), the thalamus (purple), to the hypothalamus (light blue) and through the cortex also to the amygdala from which it passes to the hypothalamus and then to response. It also goes to a a couple of other places drawn in blue, one of which has a return arrow to the amygdala, considered to be the most important region of anxiety manifestation.
The first thing to note it that there is some connection to the serotonin pathway but also note that the connection is one directional in all except on small 3rd removed from the dorsal raphne nucleus! Meaning stimulus of anxiety will enter into the serotonergic pathway but serotonin will not enter the anxiety pathways much at all it is so removed!
Anxiety is the dysfunction of a completely different hormone (neurotransmitter in the brain) called Noradrenaline (in common parlance that is adrenaline). Another picture where on a 3D image the area affected is better visible
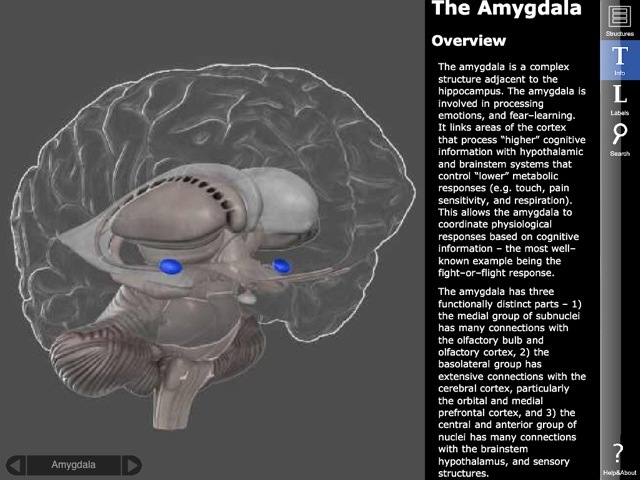
anxiety in the amygdala
On this picture above you can also read some of the descriptions about the importance of the amygdala in anxiety–marked with the two blue areas.
These pictures and analysis show that there really is no connection of significance between depression and anxiety. Most people I know who have anxiety (including me) are very happy people. There is no reason to give anti depression drugs when neither are they depressed not are they having problems with the part of the brain that needs serotonin. Why do doctors prescribe serotonin? The pharmaceuticals push the drugs. Now the FDA even approved psychotropic medications with serotonin for children as young as 8 years old, whose brains are not even developed. The damage these drugs will cause in the brains of children is unimaginable! We are creating a whole new generation of brain-damaged people!
I noted at the beginning that sometimes serotonin does work for pains, such as migraine, where depression is not present but anxiety is. How is that possible? If you read my book–noted above–you will see that the cause of migraine is the lack of voltage in certain parts of the brain. It just so happens that in a large number of cases that brain region is associated with neurons that cannot function and those are neurons that normally manufacture serotonin. If then we provide serotonin to the brain, the pain will go away since the brain now sees serotonin and it cares little about an area that is not working. Serotonin did not cure the migraine; only it temporarily filled in the gap for those neurons that would normally make serotonin and now they cannot.
Other times when the serotonin drugs don’t work, it is because the areas affected by the migraine are not located in the anatomical area where serotonin is normally made and so adding extra serotonin is not helpful. Thus the pain remains.
In conclusion: giving serotonin and SSRI drugs to a whole variety of unrelated illnesses (migraine, fibromyalgia, bipolar, anxiety, dementia, ADD, ADHD, etc.,) obviously could not be useful for treatment. Most often these drugs are prescribed off-label, which I have already complained about since that is experimenting with humans without consent.
Many doctors tell me that they do not like to prescribe anti anxiety drugs, benzodiazepines, because they are addictive and affect memory. But they forget (or shamefully perhaps don’t know) that serotonin drugs cause even more dependence, some cannot ever be stopped, and that they cause serious brain fog and memory problems and sometimes death by serotonin syndrome (toxicity).
Atypical benzodiazepine receptor ligands
I wanted to spend a moment on explaining something about Benzodiazepines that confuses most doctors–especially “atypical benzodiazepine receptor ligands.” I have been told by several psychiatrists that ligands like Ambien or Lunesta or others are not benzos and therefore they are acceptable to prescribe when they disagree with the prescription of benzodiazepines otherwise. In this section I would like to provide an explanation about what “atypical benzodiazepine receptor ligands” are and how they work because they are listed under benzodiazepines for a good reason!
The term “atypical” is probably clear; “receptor ligand” is the part that confuses many doctors because these refer to a chemical behavior that combined with the word “atypical” may suggest that these drugs are not benzos. Indeed they are not in terms of molecular structure but does that mean anything relevant? Atypical benzodiazepine ligands are listed under benzos! So how does that happen if they don’t work like benzos?
Let me quote two sentences out of a scientific research article that can be found at the NIH PubMed website if you have an account. The title of this article: Sleep pharmacology of typical and atypical ligands of benzodiazepine receptors. Not surprisingly, the following is stated in the abstract and proved all through the paper: “The results of these experiments indicate a heterogeneity in the mechanism of action of benzodiazepine and non-benzodiazepine ligands of benzodiazepine receptors, because they affect differently the various components of sleep. It is not necessary to invoke a heterogeneity of the central benzodiazepine receptors (the BZ1-BZ2 theory) in order to account for these differences, but they can be explained by the concept of spare receptors.”
So let me translate a bit so you understand what these two sentences actually mean and why they are important. In the nervous system, the neurons work by using their receptors to take in various neurotransmitters. Some of these receptors only handle one particular compound (like Oxytocin) while others, such as serotonin accept just about any molecule that is snug enough, even if not a perfect fit. When a receptor accepts a molecule of any kind, given that it is a receptor for serotonin for example, even it is has accepted a sand molecule, it activates serotonin release or blocking because the sand attached to a serotonin receptor. In other words what matters is where it connects and not what connects. This is important because of what ligands are.
Ligands are imitators and impersonators of the molecular world. Use a ligand to sleep instead of a benzo and you sleep just as well. The receptors have connected to different molecules, one to a Valium for example and in the other instance to an Ambien, but the outcome is the same: the benzodiazepne receptor was activated by the ligand and hence the brain works as if it received benzo. Doctors who believe that atypical benzodiazepine receptor ligands don’t act like benzos are mislead by the definition that simply describes their molecular structure and not what they do. They act as benzos and thus they behave and become benzos.
Do you still believe Benzodiazepines are worse than Serotonin drugs?
What is the reason for the exchange from good benzodiazepine to bad serotonin or SSRI drugs? Is it that the pharmaceuticals pay more perhaps if you prescribe those? Or are doctors not educated right? I believe that SSRIs do more damage than good. I have yet to meet a single person for whom it worked and I know thousands who take it, or used to take it. I know hundreds who are trying to quit it and are having a really difficult time. I know many who ended up with serotonin syndrome (toxic levels of serotonin) and one I knew even died. I find it amazing how clueless our medical doctors can be and still prescribe serotonin in any shape or form!
It is time we all stood up and told them that we know better! We must take our health into our hands! If we want to live to a ripe old age and have a great retirement, we better tell our doctors to stop and listen because we know the truth! No more serotonin in any form please unless it is truly indicated in “clinical depression.” In no other condition can serotonin in any shape or form be prescribed for us! And I have yet to meet a person who has the real clinical depression because chances are they are not out doing their shopping or chatting on the internet. I believe that a very large percent of the people receiving serotonin today have no clinical depression if they have depression at all!
Comments are welcome!
Angela