The latest fad of “heart healthy diet” made many people, who always had healthy diets, cut salt out of their diets–also many young children. The ones to whom the advertising campaign is aimed at, remain just as stubborn in eating whatever they want to eat and are not changing their habits. There is a question though: does salt intake directly connect to increased blood pressure? And if so how? And does reducing salt help or hurt our heart and brain or body in general. I expect you know my answer simply by how I formed the questions. I do not wish to attack those who believe low salt is heart healthy. Rather I would like to explain what heart health and diet in combination mean in terms of the human body and brain.
Since I am not a heart expert, I tell you a story of importance to guide you through my thought process. I provide my story, since I know that real well and it shocked my doctors quite a bit. Under no condition do I recommend that you drop everything and start eating salt or change your dietary habits; I merely would like to enlighten you, the reader, since if you are reading this, you have an opinion and curiosity already.
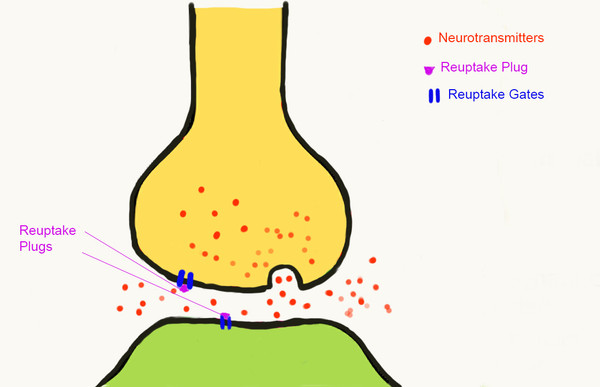
About 4 years ago I had a ton of migraines; I have had migraines for over 20 years. Otherwise I was very healthy in almost every way except for a late age asthma and the migraines. I was neither fat nor thin, had normal/low blood pressure of 110/70 to 117/78, borderline cholesterol. My family history on my mother’s side is full of hypertension and just about everyone died in or had at least one heart attack. So I thought my fate was sealed in spite of my healthy condition. But the migraines kept coming and I was referred to a migraine specialist who wanted to put me on a preventive medication, which would have been an off-label drug since it was initially created for depression. But I was not depressed plus I was told I would never be able to stop that drug in my life: it was a serotonin drug.
Being a scientist in the field of neuroscience, at that point I said “no thanks” and decided to look into this migraine business on my own–I had no salt in my mind at that time.
Of course if you look at research on migraines, nearly 100% starts with where the pain is rather than what may be the cause; perhaps because we have no easy access to see what is happening in the brain, unlike a broken arm. So my method was to look at the brain from within (in theory) based on molecular biology books I already had at home, to understand what a neuron’s requirements are for existing. Of course I learned all that in college but who pays attention? Right? We all know that the brain uses sugar for its energy but few people have asked how the neuron “opens it mouth” shall we say for simplicity to get those sugars for energy. What are the environmental requirements to the neuron to be able to energize itself? This is where I started.
To cut to the chase, I discovered a critical information that everyone in the field knows but it seems to go unnoticed or irrelevant by many. It is also complicated by the fact that not everyone has migraines given the same lack of good environment. So it is hard to say that my neurons cannot open their mouths because they don’t get enough salt at the same time as your neurons have no problem opening their mouths even though you don’t eat salt either. I now understand that migraine is genetic and a switch must turn on to activate a “migraine brain.” And the migraine brain is vastly different from the brain of a non-migraineur. The differences are greatly highlighted in my book that is sold everywhere; here I give you my publisher’s website to look inside or buy; it is available in paperback as well as digital.
Once it downed on me that the neurons in my head need to create their voltage in order to work and for that voltage they need salt, I had a life-changing moment. I hated salt all my life and I would not put it on or into nearly anything. I also drank water just as decoration and not specifically paying attention to why I did what I did. After this epiphany of salt need, I decided to give it a try. I told my doctor who nearly fainted because as you have all heard it “too much salt is bad for you.” He told me that my blood pressure will go up, it is not a good idea, etc. But if you ever had a migraine, you are ready eat rocks if people tell you they will work so I did not give a damn and started my salt increase even though I knew damned well that I have a genetic predisposition to heart problems and hypertension.
I started my morning with a pinch of salt every day with a glass of water and throughout the day I would ensure that I added extra salt to everything. For water drinking I purchased a water buzzing app on my cell phone that I set to buzz me every time I needed to drink water. Within the first months I was migraine free, by the second month migraine fog free, and after that completely migraine free.
I ate salt according to my migraine and even ate at the “very bad for your heart” M word junk food place because I knew it was high in salt. I also was told to check my blood pressure regularly and visited my doctor as well. For his and my biggest surprise, my blood pressure did not change at all; it is still around 110/70-117/78, yet on some days I eat 2-3 times the daily recommended salt while other days less.
So what is going on here? I was supposed to have an increased blood pressure–in fact I wanted to have a bit increased blood pressure since having low blood pressure can make one dizzy upon quick standing up and perhaps not so well nourished by blood through the 400 miles of blood vessels of the brain (Scientific American MIN, July/August 2014 “Out for Blood” by Elizabeth M. C. Hillman). But no matter how much salt I ate, my blood pressure did not change and my cholesterol actually dropped. I had not had as much as a cold for 3 years now, my skin got about 10 years younger, and I suddenly had a lot more energy. So where does it come from that too much salt (I mean eating 2-3 teaspoon of salt when 1 is the daily max is clearly too much) is bad for us?
I am not sure who first stated this “too much salt is bad for you” argument but it is sweeping the world in civilized countries like wildfire and the number of migraine cases are increasing exponentially as a result. So what is the connection and why did I not get hypertension in spite of the salt amount I ate?
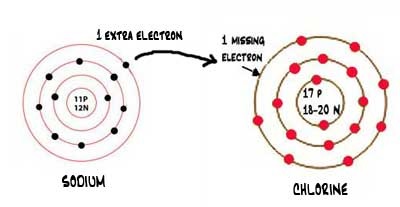
The answer is very simple: in order for your brain (or heart or lung or any cell) to open their “mouths” to feed, they need to have salt in ionic form as sodium chloride, in which sodium is NA+ and chloride is Cl- where the +/- signs represent the polarity of the ion. Sodium is inside the cell and chloride outside and with the polarity differences they attract each other through the walls of the cell, thereby providing the opportunity to the cell walls to open their mouths (sodium-potassium pumps is the official word) to take in potassium and water and spit out used toxic water. Not having voltage meant cells could not open their pumps and not having enough salt meant also not having enough sodium in the cells. Sodium retains water and this is a key important property for the body.
Since my migraines disappeared and many of my book-readers’ migraines are also gone, the question can now be addressed: how come my blood pressure did not go up (nor do my migraine book readers’ blood pressures since many contact me) and how come I am getting heart healthier with all this salt than I was without it before?! This is counter to all wisdom of today’s doctors, who will place people on sodium restricted diets rather than do the right thing: drink more water and eat more potassium if you have high blood pressure.
The reason why so many people have heart troubles as a result of too much salt is that they eat salt disproportionately to what their bodies need and they eat salt alone without enough water. If you are the type of person who puts salt and pepper on every food you get before you even taste it, there is a good chance that you will end up with a heart problem, even if you do not eat junk food.
The key to eating salt and retain heart health is to eat exactly as much salt as what your body needs to be healthy. For each individual this level is different, and each day may be different for the same individual since the level of salt one needs is dependent on many external and internal (to the body) factors: exercise, temperature, stress, illness, etc. A couch potato in a 78F temperature room sitting all day will use up way less salt than the same person sitting with friends talking or exercising, however small exercise that is. Furthermore, salt alone is bad because salt will take water wherever it can find it and will hold onto it with its life! So it is not enough to just eat salt but you must drink a lot of water as well. If you eat as much salt as your body needs and you drink as much water also as your body needs (over 70% of our body is made of this salty water), your blood pressure will not change for the worst but in fact for the better if at all. The additional benefits: lower cholesterol, younger skin, less time on the toilet since salt retains water, so you don’t have to run every time you drink water, much more energy, and stronger immune system to fight simple illnesses like a cold.
Collective benefits suggest that it is well worth taking salt in correct amount relative to the needs of each individual under serious consideration!
So is too much salt bad for you? It depends: if you drink water correspondingly with the amount of salt and potassium, no, there is no such as too much salt. If you only salt everything and finish your meal with a beer or wine, yep, too much salt will get you!
Comments are welcomed.
Angela