
You think I am joking, do you! I wrote a blog about SSRIs earlier explaining how bad they are in terms of what they do to the brain. This I did after one doctor told me that SSRIs do not increase serotonin in the brain (that doctor will be in serious trouble, rest assured!). For those who are not familiar with the acronym, SSRI stands for Selective Serotonin Reuptake Inhibitor. So let me first refresh your memories on what SSRIs do in general and how and then we will get to impotence. (I do wish someone would sue the heck out of companies making SSRIs and doctors who prescribe them since they have permanent damaging affects, do not work for 70% of the people prescribed to, and while they are supposed to only be prescribed for chronic (life long) depression, they now prescribe them for as little as being upset over a broken nail.)
If you think I sound bitchy and angry, you bet! I am! And I hope you will be too by the end of this blog!
So let me refresh the memories of those who have read my previous blog on SSRI or explain to new readers what SSRIs do and how. Here is a little drawing I created in an earlier post, recreated here for easier explanation:
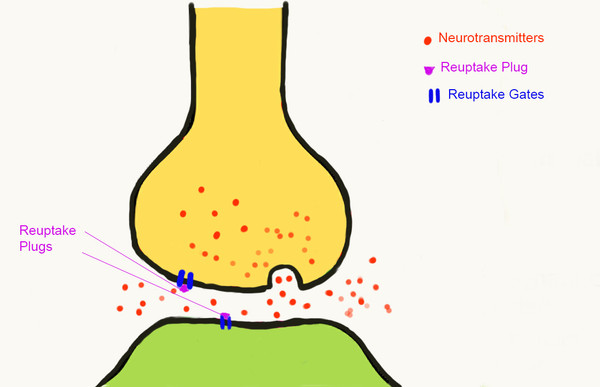
Selective Serotonin Reuptake Inhibitors in action
On the above little sketch you see two neurons (brain cells) communicating via neurotransmitters, which in this case are serotonin. Those are the red little dots. What neurons do is one kick out neurotransmitters and the neuron next to them pick those up and as a game of passing on, like in electricity, the uptaken neurotransmitter in the receiving neuron kicks a neurotransmitter out through its “foot” and sends it to the next, etc. At one point a threshold is reached by enough neurons being activated and the brain sends a message to the body “lift left leg”. It sound silly but basically this is how the brain works.
Now note the little blue gates I drew. Those are called reuptake inhibitors. Their job is to monitor when there is already enough serotonin is in the brain in that region and tell the neuron to stop making more. This is like a bathtub overflow hole. If you forget to turn the faucet off, the hole will channel the extra water back into the water system and not flood your bathroom. If you plug that hole up and forget to turn the faucet off, the tub will overflow and your bathroom will be flooded. Thus the hole has the function from preventing your bathroom from being flooded by too much water.
The reuptake inhibitors have the same job; they are the “holes” of the tub called “brain” that tell the neuron to turn the faucet off and stop making more serotonin. Serotonins are normally the plugs but here SSRIs took the plug over permanently (purple triangles). Thus when you take an SSRI, your neurons never know what they manufactured enough serotonin (there is no information about having enough) and they keep on making them until the cows come home or you die, whichever comes first. Thus if you take SSRIs, your brain is under a flow of serotonin out of control.
Serotonin has a lot of functions in the brain and in the body. In addition to mood regulation, depression, sleep, circadian rhythm, digestion, they also have functions associated with your blood flow. They can reduce blood flow also to your genitals. Yep, no blood to your genitals means impotence. No one really knew this until recently. I just read about it for the first time in the Scientific American MIND “When Arousal is Agony; Sexual Dysfunction Can Emerge When Certain Nerves Start Misfiring. Are SSRIs Partially to Blame?” by Cat Bohannon, pages 51-57, July/August 2014. This is a membership requiring article or you can just purchase the monthly issue in any store.
I am not summarizing the article but want to point out how some serious side effects can become known completely innocently unlisted by the manufacturer since the drug was never ever meant to be used for cutting blood flow! Had it not been for the few who cannot stop their erections (both male and female), the secrets of SSRI in terms of its blood flow cutting would never ever have come to the surface.
Doctors today prescribe SSRIs for children as young as 4 I believe through as old as over 100 and have no idea that they reducing blood flow not only to sexual organs but obviously to all other parts of the body, including brain!
Why is that so important you may ask? Blood carries oxygen to all parts of the body. The brain alone has 400 miles of blood vessels (yes, miles and is described in great detail in the same magazine the very next article titled “Out for Blood” by Elizabeth M.C. Hillman pages 58-65) that carry critical oxygen to the brain to all parts. Reduce the blood flow by taking SSRI and not only is your sex drive gone but so is your brain. It is literally starved of oxygen, which may cause permanent brain damage.
And this coupled with the powerful truth that once you start SSRIs your brain will have a really hard time recovering when you stop it. In some cases it cannot even recover. Thus when you stop taking SSRIs you will be suffering the consequences of SSRI withdrawal, lack of serotonin, dead neurons in the brain from not enough oxygen, and an overactive libido–just to name a few. An amazing combination that many of us would pay all of our earnings to avoid!
So before you take any SSRIs in the future, think twice. There are hundreds of different SSRI drug names so it is impossible to list them all but here are a few common ones for your reference:
- Celexa
- Lexapro, Cipraflex
- Paxil, Seroxat
- Prozac
- Luvox
- Zoloft, Lustral
- Normud, Zelmid
- Upstene
Some SNRIs that do the same but are double hits of serotonin and norepinephrine
- Pristiq
- Cymbalta
- Fetzima
- Ixel, Savella
- Elamol, Tofacine
- Effexor
Another family that are antagonist meaning they excite the receptors AND are also inhibitors of the reuptake or are modulators:
- Vibryd
- Brintellix
- Axiomin, Etonin
- Desyrel
And finally NRIs that do not work with serotonin but with Norepinephrine the same way–with similar outcomes to SSRI:
- Elavil, Endep
- Evadene
- Anafranil
- Norprami, Pertofrane
- Prothiaden
- Adapin, Sinequan
- Tofranil
- Prondol
- Feprapax, Gamanil, Lomont
- Melixeran
- Pamelor
- Vivacil
- Surmontil
- Insidon
- Stablon
- Survector, Maneon–this also worked on dopamine receptors but has been taken off the market since
These are just some of the most common brand names–when you see more than one in a line it means that in other countries they may go by those other names. Generics exist by the gazillion so those are not listed. You need to watch out for your health!
Migraine and Fibromyalgia patients!
A special caution I want to add here for those who receive SSRIs for their migraines of fibromyalgia. Many doctors today prescribe SSRIs as preventative for migraine patients without even checking their blood pressure. I am not nearly as familiar with fibromyalgia since I do not have that illness and thus was never prescribed anything for it but as I read from my migraine readers who also have fibromyalgia, SSRIs are also common in practice for that.
Please be aware that if your blood pressure is already low, that means your blood already has a hard time traversing the 400 miles of vessels in your brain. Add to that an SSRI and you are going to be in serious trouble.
I also read from many of my UK migraineurs that in the UK they prescribe beta blockers to lower the blood pressure regardless of what the blood pressure is–and for most migraineurs it is already low. If they also prescribe an SSRI, you potentially are in grave danger of dizziness, fainting, hemiplegic migraines, etc. I now understand the connection!
Please avoid taking any SSRIs if possible! If you have migraines, we already have a solution for that; please read my book. I am now working toward finding solutions to fibromyalgia but I am not there yet! However, cutting the blood supply to any part of your body cannot be a good thing under any condition so please do not start taking an SSRI!
Comments are welcome!
Angela


I received a comment on this article from g+ so I want to post the question and also my answer so you can see what people have in mind and also so I remember what was said and what I answered.
The question: by Mr. Watts: does it have connection to MSA-P? not the jokes lol
My answer:
MSA-P as in Parkinson’s disease type multiple system atrophy? I suppose it can because serotonin has a lot to do with blood pressure regulation, one of the things that break down in MSA-P. But MSA-P is a cell degenerative disease whose cause is not yet known and not even understood. Various different drug trials have failed and some showed some signs of improvement. SSRI will not stop the progression of the disease since it is only meant to benefit depression–which may very well be a side effect of MSA-P–but even for depression, it only works for 30% of the cases. It is really not sure if SSRI really benefits anything and anyone from my reading of research papers and analysis but it can permanently damage brain cells on its own. If I had the say, I would remove all SSRIs from the market since they are being used on patients with a wide range of illnesses off label as experiments without written consent.
For example giving them for migraine was (and may still be) off-label prescription since the drug is originally made for depression and not as a pain killer. They also give it to people with OCD, bipolar, depression, ADD, ADHD, yet few similarities exists between a depression and an ADHD patient (in fact they are polar opposites!)… so why the same drug? No idea–it is easy I guess.
Plus serotonin syndrome increases each year (serotonin syndrome = serotonin toxicity) which is deadly if not caught early. NIH literature says that only 15% of doctors recognize serotonin syndrome and that 15% in 2012 (last US record) showed about 80,000 people getting it, nearly 8,000 very serious–meaning they caught is a bit later than within the first 24 hours–and nearly 100 people died. And this represents the 15% of doctors who recognize it. The 85% also probably had proportionate number of people with serotonin syndrome, only called it “hospital delirium” or “drug induced delirium” or “dementia” or “Alzheimer’s type dementia” or “schizophrenia,” etc. So if I include them as well, we probably had close to half a million cases in the US in 2012 and over 700 death.
I am not sure what the explanation would be to prescribe it for MSA-P since for Parkinson’s in general they suspect the dopamine pathways to be in trouble and not serotonin and the walking problems are trouble with the cells in the cerebellum, which control automatic function, such as walking, where there are no serotonin releasing neurons much if at all–not all is yet known since multiple neurotransmitters are released by a ton of neurons… It is something you should check into if that is what you have been prescribed. Also note that you cannot cut SSRIs cold turkey… you need to get off very slowly and if you have been on it for a long time, you may never be able to get off of it. Talk to your doctor and find out why, what, how, and options. I hope this helps!
LikeLike